A Brief History of Human Disease Genetics
From Mendel’s laws of inheritance to genome sequencing, artificial intelligence, and precision medicine
Why do some diseases appear repeatedly across generations, while others emerge through a complex interplay of thousands of subtle inherited factors and environmental influences? This question has shaped one of the most important scientific journeys in modern medicine. Over the past century and a half, human disease genetics has progressed from careful observation of family traits to genome-wide sequencing, population biobanks, computational prediction, and targeted molecular therapies.
Today, genetics is no longer a niche specialty. It influences oncology, cardiology, neurology, reproductive medicine, pharmacology, rare disease diagnostics, and preventive healthcare. Modern medicine increasingly depends on understanding how inherited variation influences biological pathways, disease susceptibility, treatment response, and long-term outcomes.
Based on the landmark Nature review “A brief history of human disease genetics”, this article explores the major scientific eras, conceptual breakthroughs, clinical transformations, and future directions that have defined the field.
McCarthy MI, MacArthur DG, et al. A brief history of human disease genetics. Nature (2019) 🔗
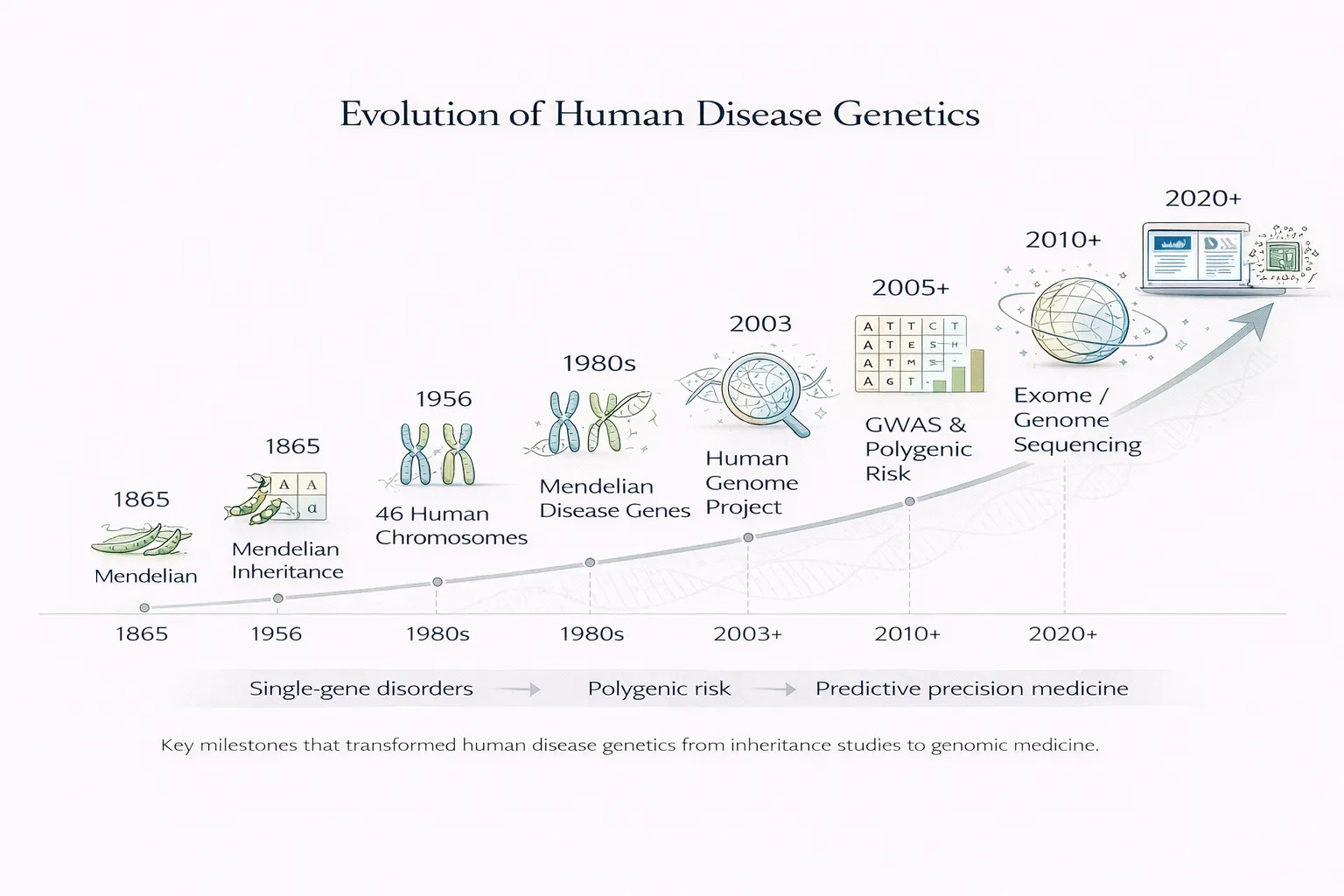
Timeline of Human Disease Genetics
| Era | Milestone | Clinical Impact |
|---|---|---|
| 1865 | Mendel’s laws of inheritance | Foundation of heredity |
| Early 1900s | Human pedigree genetics | Family risk prediction |
| 1956 | 46 human chromosomes defined | Cytogenetic diagnosis |
| 1980s–1990s | Positional cloning | Mendelian disease genes identified |
| 2003 | Human Genome Project | Modern genomics begins |
| 2005+ | GWAS era | Polygenic common disease risk |
| 2010+ | Exome/genome sequencing | Rare disease diagnosis revolution |
| 2020+ | AI + multi-omics | Precision medicine at scale |
Why This History Matters Today
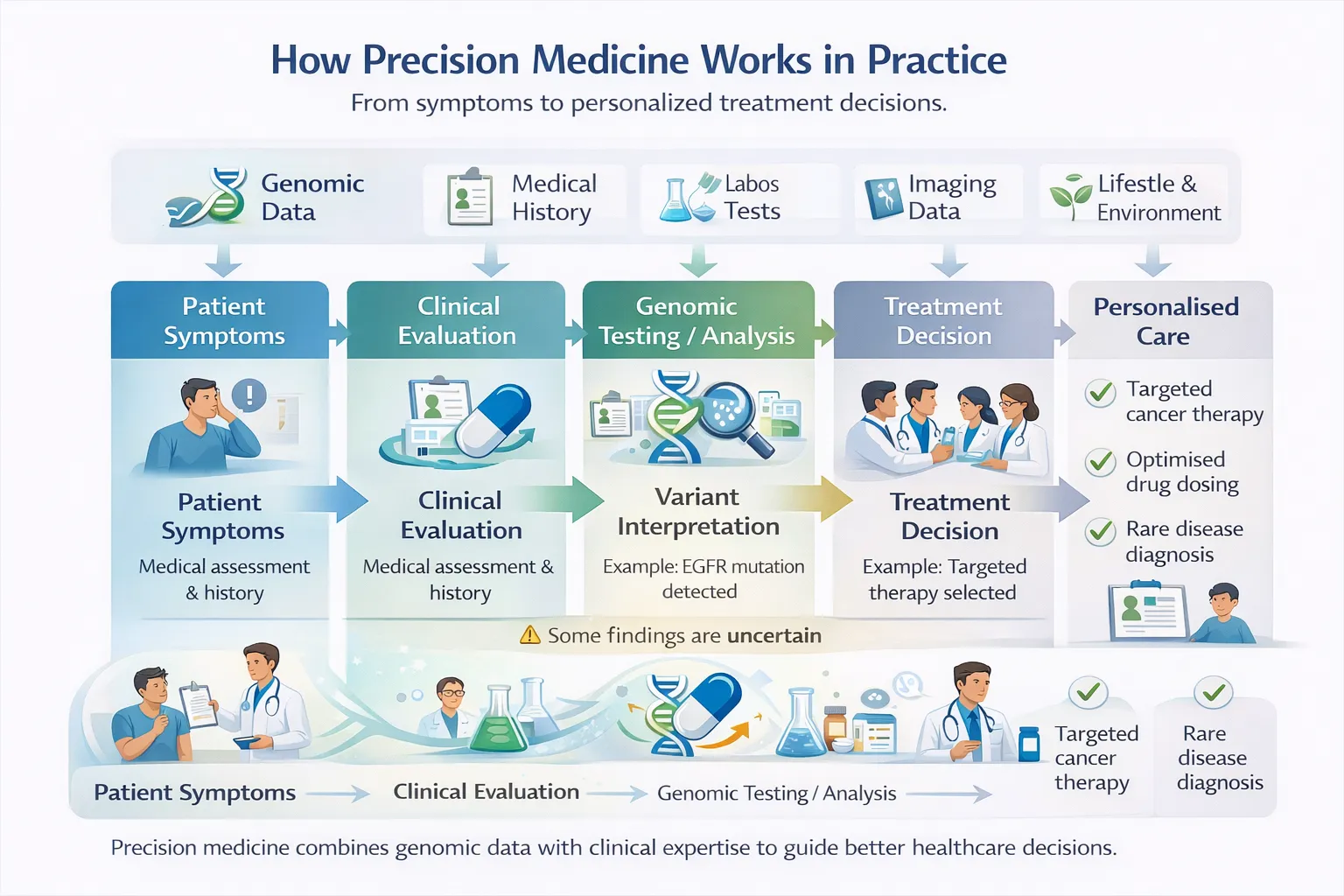
The history of disease genetics is not simply an academic narrative—it directly underpins modern healthcare. Many clinical decisions now depend on genomic information, whether identifying a hereditary cancer syndrome, diagnosing a child with a rare developmental disorder, choosing a targeted oncology drug, or estimating inherited cardiovascular risk.
Genetics has also transformed how diseases are conceptualized. Conditions once grouped solely by symptoms are now being subdivided by molecular cause. Conversely, diseases affecting different organs may share common biological pathways. This transition from descriptive medicine to mechanistic medicine is one of the defining shifts of the twenty-first century.
Understanding the history of disease genetics helps explain why precision medicine is now possible—and why the next phase of medicine will likely be increasingly genomic, computational, and individualized.
1. Foundations: Recognizing Heredity in Disease
Long before genes, chromosomes, or DNA were understood, physicians recognized that certain disorders clustered in families. Historical records described inherited bleeding disorders, neurological diseases, pigment disorders, and congenital anomalies that recurred across generations. These observations suggested that disease risk could be transmitted biologically rather than arising purely from environment or chance.
However, there was no robust scientific framework to explain inheritance. Ideas ranged from blending theories to vague notions of familial constitution. The turning point came through the work of Gregor Mendel, whose experiments in pea plants demonstrated that traits are inherited through discrete units that segregate according to predictable mathematical rules.
Mendel’s insights were revolutionary because they introduced several enduring principles:
- Inheritance is particulate rather than blended
- Traits can skip generations
- Predictable ratios emerge across offspring
- Dominance and recessiveness influence phenotype
Although Mendel did not study human disease, his framework ultimately became the intellectual foundation of medical genetics.
2. Mendelian Medicine and Human Pedigrees
Once Mendelian principles were rediscovered and applied to humans in the early twentieth century, medicine gained one of its first predictive tools: pedigree analysis. By systematically mapping disease across generations, clinicians could infer patterns of inheritance and estimate recurrence risk.
This led to the classification of several major inheritance modes:
- Autosomal dominant, where one altered copy is sufficient to cause disease
- Autosomal recessive, where two altered copies are required
- X-linked, where variants on the X chromosome often disproportionately affect males
- Mitochondrial, where maternal inheritance reflects mitochondrial DNA transmission
Pedigree analysis transformed clinical care. Families affected by Huntington disease, Duchenne muscular dystrophy, hemophilia, or inherited blindness could receive more accurate counseling regarding future offspring and relatives.
Classic examples included:
- Huntington disease
- Duchenne muscular dystrophy
- Hemophilia
- Cystic fibrosis
Importantly, pedigree-based genetics also revealed that some diseases followed clear Mendelian patterns while others did not. This distinction foreshadowed the later separation between monogenic and complex disease genetics.
3. Cytogenetics: Disease at the Chromosome Scale
The next major leap occurred when disease was linked not only to invisible hereditary factors but to visible chromosome abnormalities. After the normal human chromosome number was correctly established as 46 in 1956, chromosomal disorders could be identified systematically.
This immediately transformed diagnosis. Conditions such as Down syndrome were shown to result from trisomy 21, while Turner syndrome and Klinefelter syndrome reflected sex chromosome aneuploidies. In cancer biology, structural rearrangements and translocations became recognized as important drivers of malignancy.
Cytogenetics introduced a profound new concept: disease can arise from changes in genome structure and gene dosage, not only from sequence-level mutations. This era laid the groundwork for several modern technologies:
- Karyotyping
- Fluorescence in situ hybridization (FISH)
- Chromosomal microarray analysis
- Structural variant detection in sequencing pipelines
It also established cancer as a genetic disease at the chromosomal level, paving the way for molecular oncology.
This era introduced a crucial concept:
Disease can arise not only from sequence changes, but from altered gene dosage and genome structure.
Cytogenetics laid the groundwork for modern chromosomal microarray testing and cancer genomics.
4. Molecular Genetics and the Gene Discovery Revolution
From the 1970s through the 1990s, recombinant DNA methods, linkage mapping, and positional cloning enabled direct identification of disease-causing genes. For the first time, researchers could move from observing inheritance patterns to pinpointing the exact molecular lesions responsible.
Landmark discoveries included:
- HBB mutations causing sickle cell disease
- CFTR causing cystic fibrosis
- DMD causing Duchenne muscular dystrophy
- HTT causing Huntington disease
- BRCA1/2 associated with hereditary breast and ovarian cancer
Why This Changed Medicine
This transformed medicine in several ways. Diagnosis became molecular rather than purely clinical. Carrier testing became feasible. Relatives could undergo cascade screening. Researchers could study disease pathways directly. Therapeutic development became more rational because causal genes were known.
Perhaps most importantly, molecular genetics established that understanding DNA sequence could reveal both disease mechanism and clinical strategy. For the first time, clinicians could move from symptom-based diagnosis to molecular diagnosis.
This enabled:
- Confirmatory testing
- Carrier detection
- Family cascade screening
- Mechanistic understanding
- Therapeutic targeting
5. Rare Diseases, Rare Variants
Rare disease genetics represents one of the clearest success stories in human genomics. Although each rare disorder individually affects relatively few patients, rare diseases collectively affect millions worldwide and often impose severe lifelong burdens.
Many rare disorders are caused by rare variants of large effect, often within a single gene. These variants may disrupt protein coding sequence, alter splicing, truncate transcripts, or affect dosage through copy-number changes. Because effect sizes are often substantial, the causal relationship between genotype and phenotype can be comparatively direct.
Why Rare Disease Genetics Works So Well
Historically, gene discovery relied on large pedigrees and linkage studies. This was powerful but slow. The arrival of whole-exome sequencing (WES) transformed the field by enabling rapid identification of coding variants across nearly all genes. Later, whole-genome sequencing (WGS) expanded detection into non-coding regions, structural variation, repeat expansions, and complex rearrangements. These variants often show:
- High penetrance
- Clear inheritance patterns
- Strong causal links to phenotype
- Large effect sizes
This makes gene discovery highly informative. This revolution has been especially important for:
- Developmental delay and intellectual disability
- Congenital anomalies
- Pediatric epilepsy and neurology
- Inherited metabolic disease
- Ultra-rare syndromes with unclear clinical presentation
Rare disease genetics has also had broader scientific impact. Genes first discovered in rare syndromes often illuminate pathways relevant to common disease. For example, rare lipid disorders have clarified cholesterol metabolism, and monogenic diabetes has reshaped understanding of insulin biology.
Thus, rare disease research frequently generates insights far beyond the rare disease community itself.
6. Common Diseases, Common Variants
While Mendelian disorders are often driven by single high-impact variants, common diseases such as type 2 diabetes, coronary artery disease, asthma, obesity, and schizophrenia usually arise through a much more distributed architecture.
These diseases are often polygenic, meaning risk is influenced by many variants, each contributing a small effect. Environmental exposures, aging, lifestyle, infection, and socioeconomic context may further modify outcomes.
GWAS Changed the Field
The major methodological breakthrough in this area was the rise of genome-wide association studies (GWAS). Rather than testing one gene at a time, GWAS scans the genome for statistical associations between common variants and disease across large populations.
GWAS fundamentally changed human genetics by demonstrating that:
- Most common disease risk is highly polygenic
- Many risk variants lie in regulatory rather than coding regions
- Biological pathways can be discovered even when individual effects are small
- Large sample sizes are essential for complex trait discovery
This shattered the old one-gene-one-disease mindset.
Examples of GWAS Impact
GWAS uncovered important biology in:
- Type 2 diabetes
- Lipid metabolism
- Autoimmune disease
- Obesity
- Psychiatric disorders
Polygenic Risk Scores
One downstream application has been the development of polygenic risk scores (PRS), which aggregate many variants to estimate inherited susceptibility. While still evolving clinically, PRS may contribute to earlier prevention, screening personalization, and refined risk stratification.
Rare vs Common Disease Genetics
| Feature | Rare Disease Genetics | Common Disease Genetics |
|---|---|---|
| Variant Frequency | Rare | Common |
| Effect Size | Large | Small |
| Inheritance | Often Mendelian | Polygenic |
| Main Tools | WES / WGS | GWAS |
| Examples | CF, DMD, SMA | Diabetes, CAD, Asthma |
7. Genotype–Phenotype Maps
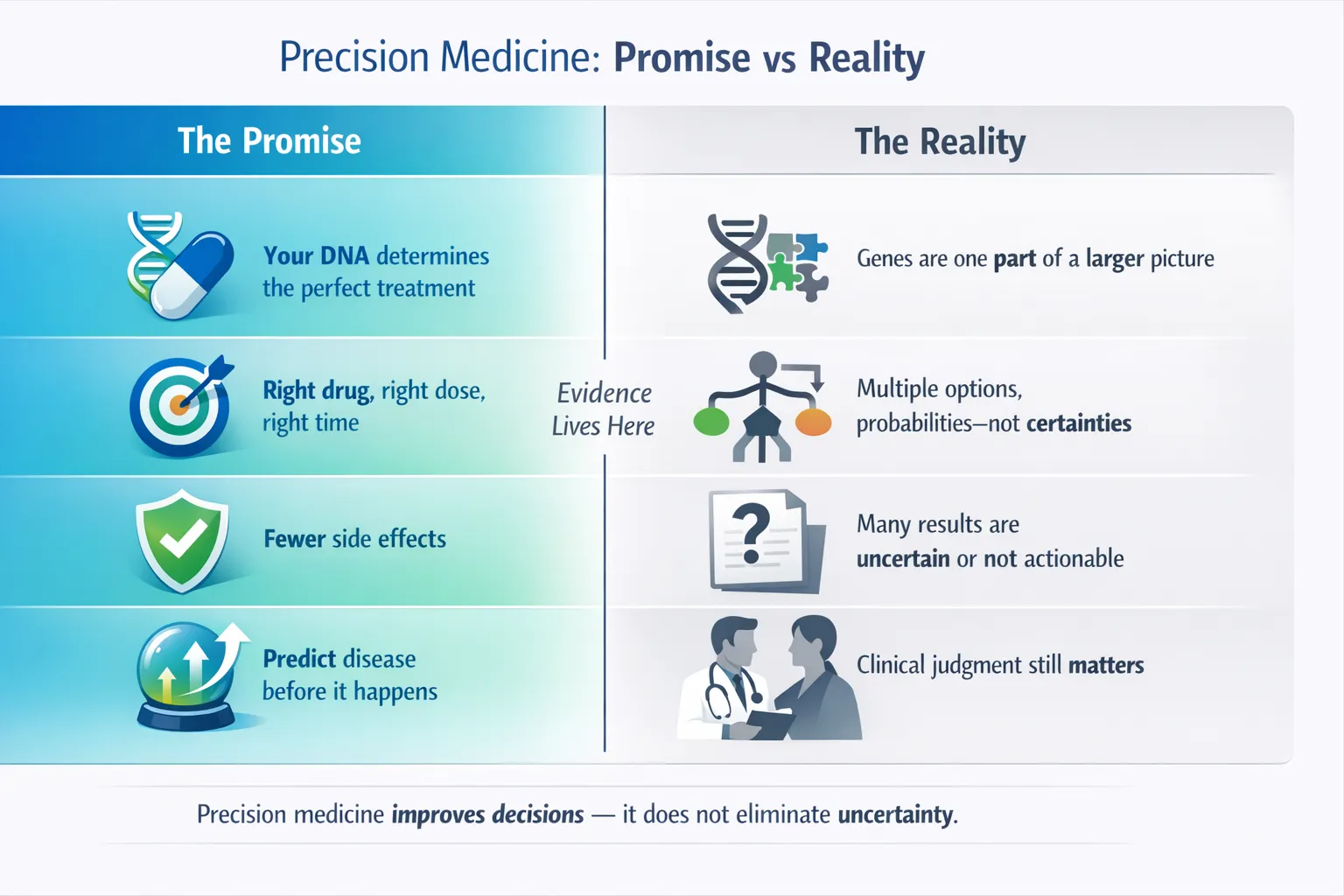
A central challenge in genetics is understanding how sequence variation translates into biological and clinical outcomes. This is the problem of genotype–phenotype mapping, and it is often more complex than early genetic models suggested.
Why It Is Complex
The same pathogenic variant may cause severe disease in one individual and mild manifestations in another. Different genes may produce clinically similar syndromes. Additional variants elsewhere in the genome can modify severity. Environmental exposures such as diet, toxins, infections, exercise, or aging may further influence penetrance.
This means genotype does not always map cleanly to phenotype.
- One Genotype, Many Phenotypes
- The same mutation may produce different severity across individuals.
- Different genes may cause the same syndrome.
- Modifier Effects and variants can worsen or buffer disease.
- Diet, infection, toxins, exercise, and aging influence penetrance.
Why This Matters
Improved genotype–phenotype maps are crucial because they support:
- More accurate variant interpretation
- Better prognosis estimation
- Molecular disease subtyping
- Precision trial enrollment
- Therapeutic target prioritization
As sequencing becomes easier, interpretation increasingly becomes the true bottleneck.
8. Human Genome Project: Infrastructure for Modern Medicine
The Human Genome Project (HGP), completed in the early 2000s, provided the reference framework that underlies nearly all modern genomic medicine. While often described as a sequencing achievement, its deeper significance was infrastructural.
The HGP enabled:
- Standardized genomic coordinates
- Comprehensive gene catalogs
- Comparative genomics across species
- Efficient mapping of new variants
- Improved annotation pipelines
Without a shared reference genome, today’s diagnostic sequencing, cancer panels, variant databases, and research pipelines would be far more limited.
The HGP also helped catalyze cost reductions and technology development that made large-scale sequencing clinically realistic.
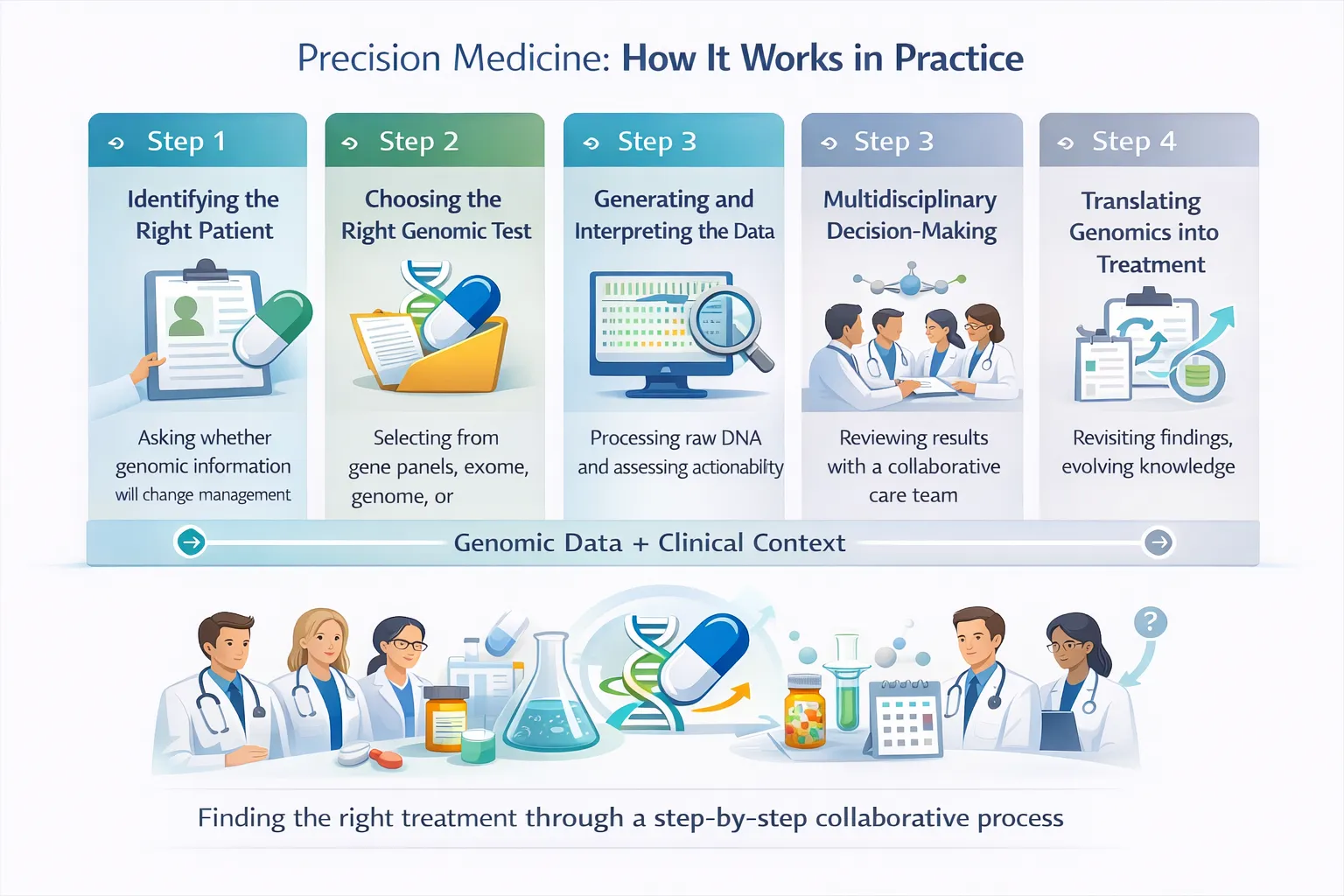
9. Clinical Implementation of Human Genetics
Human disease genetics has now moved from research into routine care.
In oncology, inherited testing for genes such as BRCA1/2 guides surveillance and preventive decisions, while tumor sequencing increasingly directs targeted therapies and trial eligibility.
In cardiology, genetic testing helps diagnose inherited arrhythmias, cardiomyopathies, and familial hypercholesterolemia, often enabling screening of relatives after sudden cardiac events.
In endocrinology, recognition of monogenic diabetes can dramatically alter treatment selection compared with standard type 1 or type 2 paradigms.
In rare disease medicine, exome and genome sequencing have shortened diagnostic odysseys that previously lasted years.
In reproductive medicine, carrier screening, prenatal testing, and embryo testing have expanded reproductive choice and early diagnosis.
In pharmacogenomics, inherited variants affecting drug metabolism (CYP-mediated metabolism) or toxicity (Drug toxicity risk variants) increasingly inform prescribing decisions.
These examples demonstrate that genetics is no longer peripheral—it is becoming embedded within multiple clinical specialties.
10. Disease Reclassification Through Genetics
Historically, diseases were grouped by symptoms, pathology, or affected organ system. Genetics has shown that this framework is often incomplete.
Patients with similar symptoms may have entirely different molecular causes requiring different treatments. Conversely, diseases affecting distinct tissues may share convergent pathways.
Examples include:
- Molecular subtypes of cancer with distinct therapies
- Monogenic diabetes previously mislabeled as type 1 or type 2
- Genetically heterogeneous cardiomyopathies requiring different management approaches
This shift marks the emergence of mechanistic taxonomy, where disease categories increasingly reflect biology rather than appearance alone.
11. Three Lessons from the History of Disease Genetics
The first lesson is that biology is more complex than expected. Mendelian models remain powerful, but many diseases involve polygenic architecture, environmental interactions, mosaicism, and dynamic regulatory networks.
The second lesson is that scale changes discovery. Large biobanks, population sequencing, and integrated datasets have accelerated progress far beyond what small family studies alone could achieve.
The third lesson is that diagnosis is becoming intervention. Genetic insight increasingly informs treatment selection, prevention, and even direct molecular correction.
12. Looking Forward
The next phase of disease genetics may be even more transformative than the last.
- Multi-omics medicine aims to integrate genomics with transcriptomics, proteomics, metabolomics, and epigenomics to understand disease systems more completely.
- Artificial intelligence may improve variant classification, imaging-genomic fusion, therapeutic discovery, and individualized risk modeling.
- Massive linked biobanks that connect genomes with longitudinal health records can reveal lifetime disease trajectories and treatment responses.
- Genome editing technologies such as CRISPR may shift genetics from prediction toward correction.
- Precision prevention could use inherited risk to guide earlier intervention before disease develops.
- Equity and diversity will be essential, as genomic medicine must represent global populations to be accurate and fair.
13. Persistent Challenges
Despite progress, major barriers remain:
- Much heritability for common disease is still unexplained
- Non-coding variants are difficult to interpret mechanistically
- Penetrance varies widely
- Gene–environment interactions are complex
- Data privacy and governance require careful stewardship
- Access to genomic medicine remains unequal across regions and health systems
These are not peripheral issues—they define the next frontier of responsible genomic medicine.
14. Conclusion
The history of human disease genetics is a progression from observation to explanation, from explanation to prediction, and from prediction toward intervention.
We moved from family pedigrees…
- to chromosomes…
- to genes…
- to genomes…
- to population-scale biology.
Today, genetics no longer sits at the edge of medicine—it is becoming part of medicine’s core operating system.
The next chapter will likely unite genomics, AI, functional biology, and gene editing into a new era of precision healthcare.
Explore related insights
- Trends in Clinical Genetic Testing
- Integrating Genomics into Multimodal EHR Foundation Models
- Prime Editing: Advances in Human Gene Therapy
- Past, Present, and Future of CRISPR Genome Editing Technologies
- Single-Cell Multi-omics Technologies