Introduction
From first-in-human genome editing studies to next-generation targeted delivery platforms
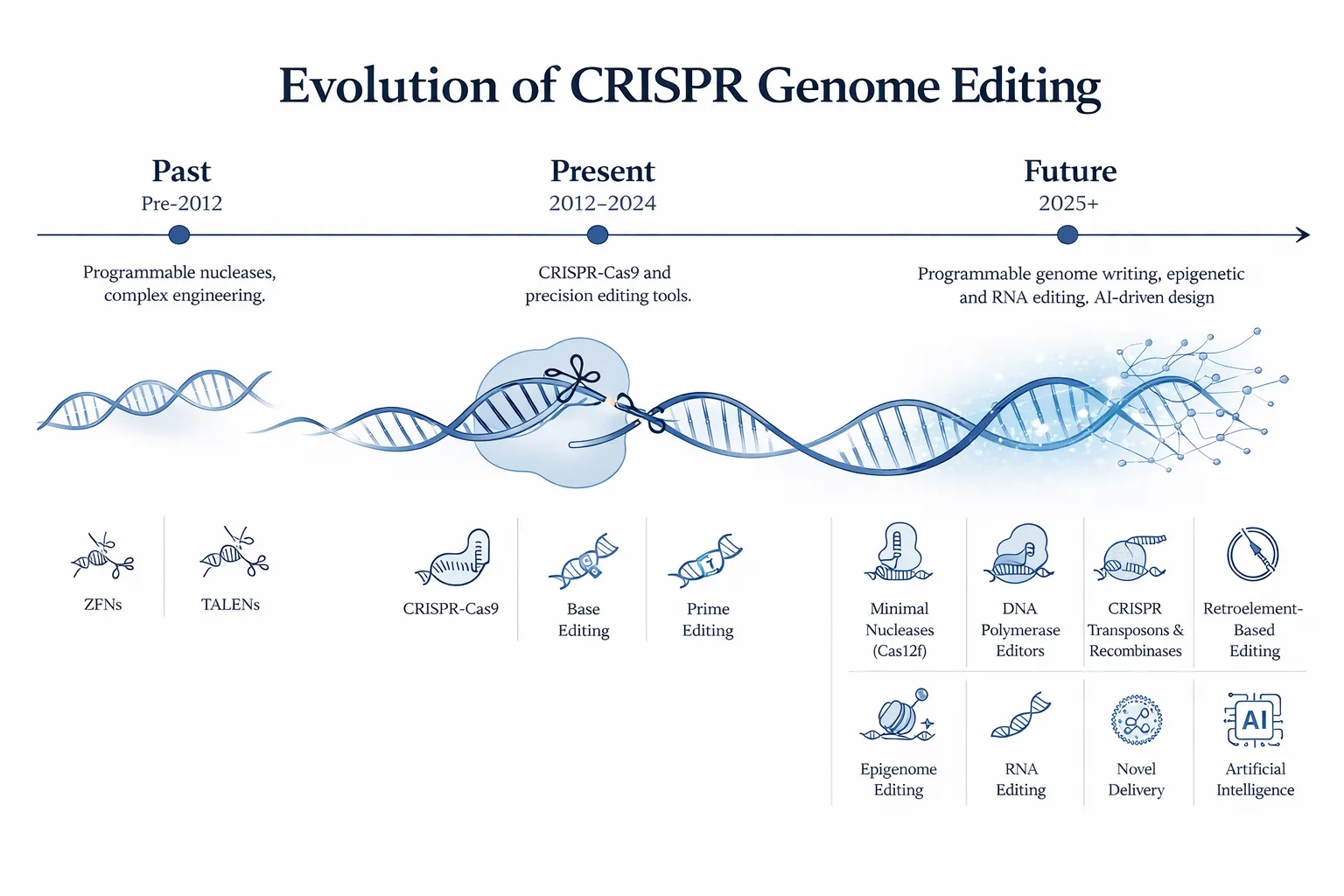
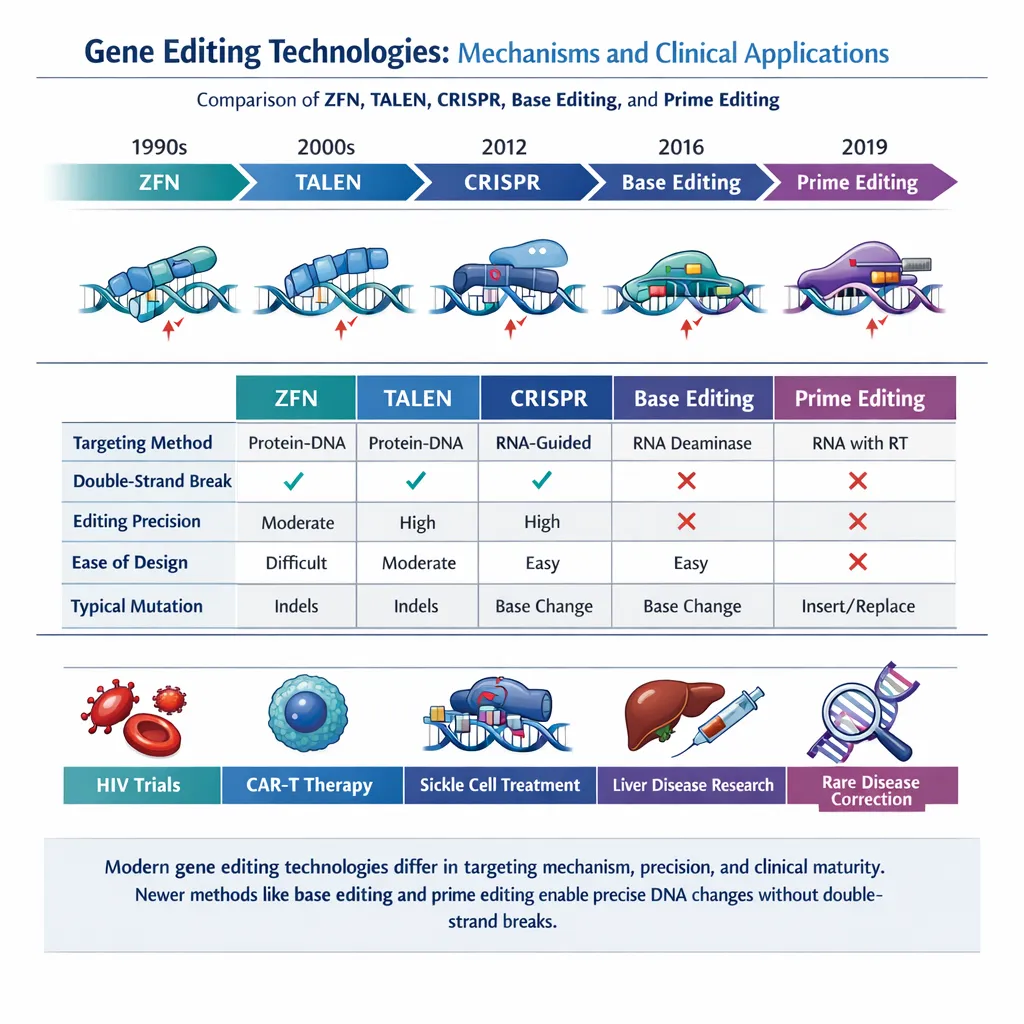
Gene editing has entered a decisive translational phase. What began as a set of programmable molecular tools for manipulating DNA is now becoming a therapeutic platform capable of addressing inherited disease, cancer, and complex acquired disorders. CRISPR-Cas systems, base editors, prime editors, zinc-finger nucleases, TALENs, and RNA-guided transposon systems have dramatically expanded the ways in which genomes can be modified. Yet despite this progress, the rate-limiting step in many therapeutic programs is no longer editor design itself—it is delivery.
To achieve clinically meaningful benefit, editing machinery must be transported to the correct cells, internalized efficiently, released intracellularly, and expressed or activated for an appropriate duration. Delivery systems must simultaneously balance potency, specificity, manufacturability, tolerability, and cost. This challenge becomes even more complex when moving beyond the liver or blood system into tissues such as skeletal muscle, lung, retina, heart, or central nervous system.
Recent publications in Molecular Therapy: Nucleic Acids emphasize that successful gene editing medicines arise from the intersection of two engineering problems: precise editing chemistry and clinically viable delivery technology. The field is therefore shifting from pure molecular biology toward integrated therapeutic systems design.
Why Delivery Has Become the Central Challenge in Gene Editing
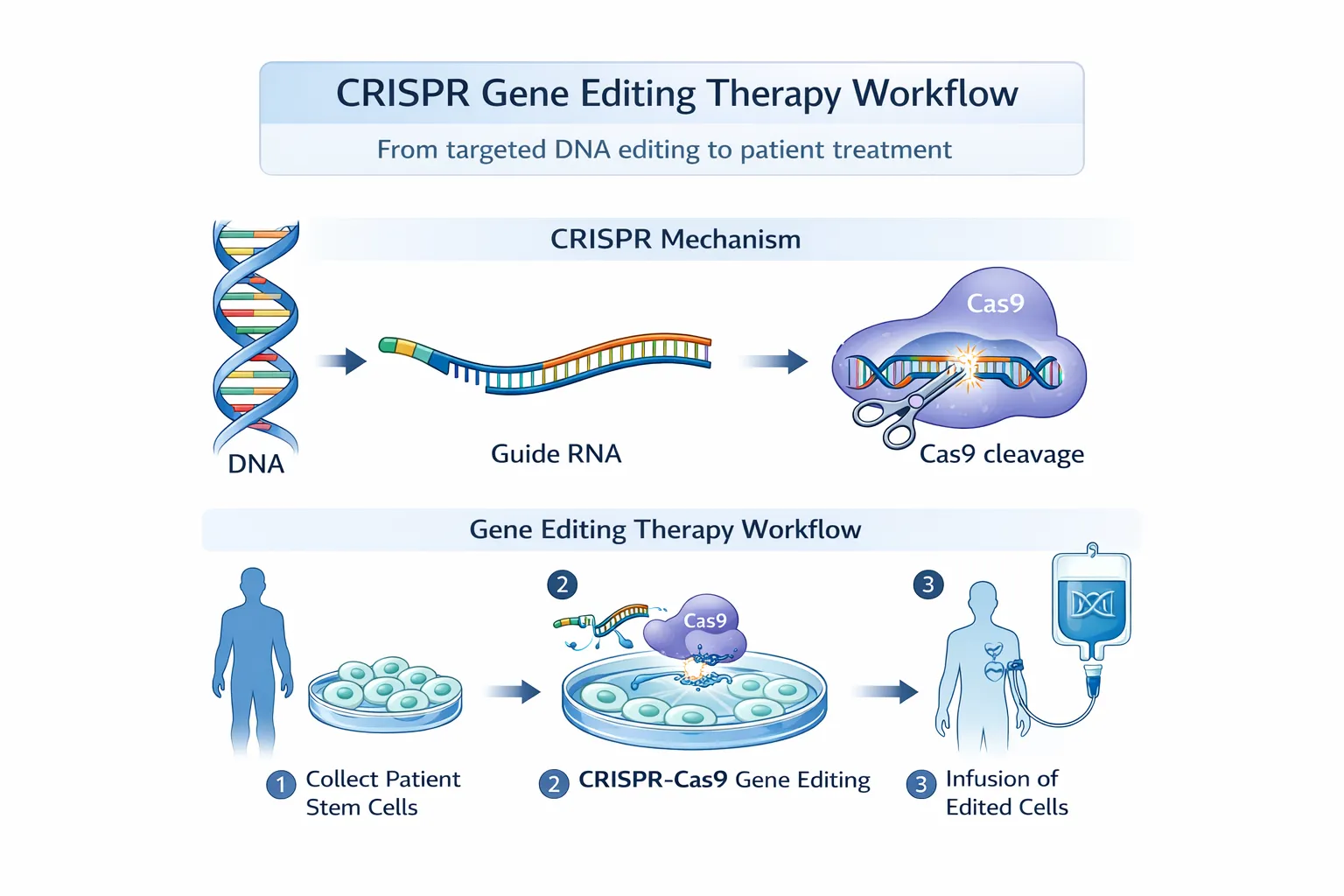
Genome editors are highly sophisticated molecular machines, but they are only effective when they reach the appropriate intracellular compartment in sufficient quantity. A CRISPR nuclease requires a guide RNA and a catalytic protein or encoded mRNA. Base editors and prime editors are even more demanding because they often involve larger fusion proteins, more complex guide architectures, and tighter expression windows.
In therapeutic settings, these components encounter multiple barriers before they can function. Systemically administered materials must survive circulation, avoid rapid renal or hepatic clearance, evade immune recognition, traverse vascular barriers, enter target cells, and escape endosomes after uptake. For DNA editing applications, they must also access the nucleus. Each step can dramatically reduce efficiency.
Delivery also influences safety. Excessive exposure of non-target tissues can produce unintended editing or toxicity. Persistent expression from integrating or long-lived vectors may increase the risk of off-target events. Conversely, transient delivery may improve safety but reduce efficacy if intracellular dosing is insufficient. Thus, the delivery platform largely determines the therapeutic index of a gene editing medicine.
This explains why many of the most important innovations in the field today concern nanoparticle chemistry, viral capsid engineering, targeting ligands, dosing strategy, and cargo architecture rather than nuclease discovery alone.
Clinical Trial Landscape for Gene Editing Therapies
Clinical gene editing has progressed rapidly from proof-of-concept studies to late-stage therapeutic programs. Early clinical success has largely come from indications where cells can be manipulated outside the body or where delivery naturally concentrates in accessible organs such as the liver.
Hematology has emerged as one of the leading therapeutic areas because hematopoietic stem and progenitor cells can be harvested, edited ex vivo, and reinfused following quality control. This strategy has been particularly important for hemoglobinopathies such as sickle cell disease and beta-thalassemia, where edited stem cells can repopulate the bone marrow and produce durable benefit.
The liver has become the leading target for systemic in vivo editing because intravenously administered nanoparticles and some viral vectors naturally accumulate in hepatocytes. This has accelerated programs in transthyretin amyloidosis, metabolic disorders, and lipid metabolism.
Ophthalmology represents another important frontier. The eye is relatively accessible, compartmentalized, and partially immune privileged, making it well suited to local administration strategies. Retinal disorders caused by well-defined genetic lesions are therefore attractive targets.
Oncology has adopted gene editing through a different route: engineering immune cells. Rather than editing diseased tissue directly, CRISPR tools are used to modify T cells, NK cells, or other cellular therapies to improve tumor recognition, persistence, and resistance to immunosuppressive microenvironments.
As the field matures, clinical development is broadening from monogenic diseases toward complex tissue disorders and combination therapeutic strategies.
Ex Vivo Gene Editing: The First Wave of Clinical Translation
Ex vivo editing has delivered some of the clearest clinical successes because it separates genome engineering from the complexity of systemic delivery. Cells are collected from the patient, edited under controlled manufacturing conditions, tested extensively, and then returned.
This approach provides several advantages. Investigators can optimize transfection conditions, enrich successfully edited cells, evaluate genomic integrity, and remove nonviable or poorly edited populations before infusion. The patient is not directly exposed to high systemic levels of editor cargo, which can reduce toxicology concerns.
For hematologic disease, ex vivo editing has been transformative. In sickle cell disease and beta-thalassemia, strategies often focus on disrupting repressors of fetal hemoglobin or directly correcting pathogenic mutations. Because corrected stem cells self-renew, a single successful intervention may provide long-term therapeutic benefit.
In oncology, ex vivo editing enables multiplex engineering of immune cells. CRISPR can remove endogenous T-cell receptors, insert chimeric antigen receptors, disrupt checkpoint pathways, or enhance resistance to tumor-mediated suppression. These strategies are particularly attractive for creating standardized allogeneic cell therapies.
The main limitation of ex vivo editing is biological scope. Only certain cell types can be reliably harvested, manipulated, expanded, and returned. This excludes many organs such as brain, heart, and skeletal muscle, where in vivo delivery remains essential.
In Vivo Gene Editing: Expanding Therapeutic Reach
In vivo editing aims to deliver genome engineering cargo directly into tissues inside the patient. This model is more scalable than individualized ex vivo manufacturing and may ultimately reach a broader range of diseases. However, it is substantially more complex.
When editing is performed in vivo, the delivery system must solve biodistribution, cellular uptake, intracellular release, and dose control simultaneously. It must also avoid immune activation and minimize exposure to unintended tissues.
Despite these challenges, in vivo editing offers enormous potential. It can target organs that are inaccessible to cell harvesting approaches, simplify treatment logistics, and allow repeatable dosing if the delivery vehicle supports re-administration.
The earliest successes have largely involved liver-directed therapies because hepatocytes are naturally accessible to lipid nanoparticles and some viral systems. The next major frontier is extrahepatic delivery—reaching muscle, lung, CNS, kidney, and immune compartments with equal precision.
Progress in this area will likely determine whether gene editing becomes a niche therapy for selected diseases or a broadly deployable therapeutic class.
Major Delivery Systems for Gene Editing
Viral Vectors
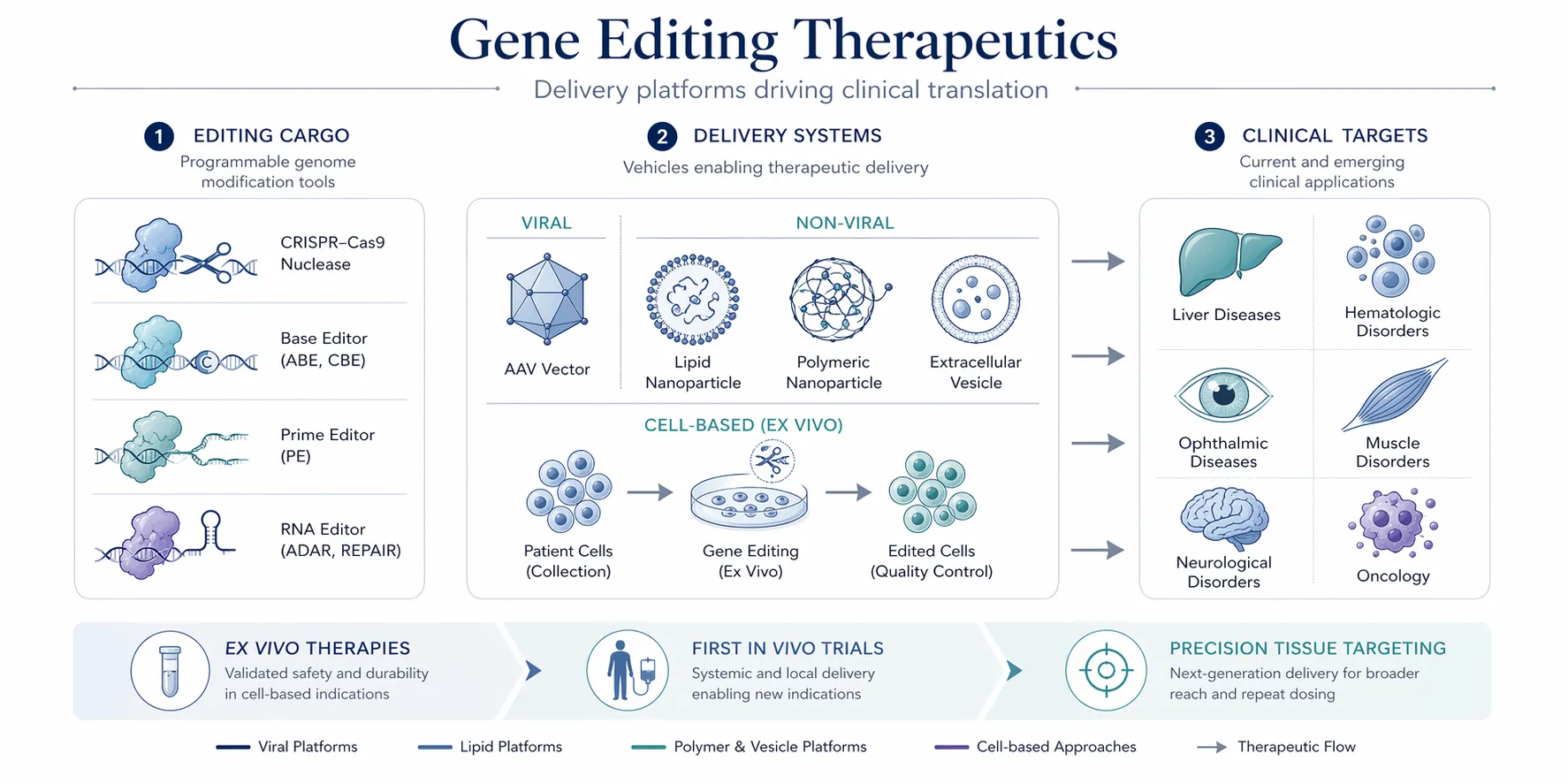
Viral vectors, especially adeno-associated virus (AAV), have played a foundational role in genetic medicine and remain highly relevant for gene editing. AAV offers efficient gene transfer, multiple serotypes with distinct tissue tropisms, and strong in vivo transduction in tissues such as retina, muscle, and liver.
For editing applications, AAV can deliver DNA encoding nucleases, guides, or donor templates. This can be useful when prolonged expression is needed, but sustained editor expression may also increase the probability of off-target activity. AAV is further constrained by limited packaging capacity, which creates challenges for large editors such as base editors or prime editors.
Another major issue is immunity. Many individuals possess pre-existing antibodies to AAV, and repeat dosing can be difficult after initial exposure. Nevertheless, AAV remains an important modality, particularly for localized or tissue-specific applications where durable transduction is beneficial.
Lipid Nanoparticles (LNPs)
Lipid nanoparticles have emerged as one of the most important non-viral delivery systems in modern therapeutics. Their success in RNA medicine has accelerated adoption for genome editing applications, particularly because they can deliver mRNA encoding editors together with guide RNAs.
A major advantage of LNPs is transient expression. Instead of continuously expressing editing machinery from DNA vectors, mRNA-based systems typically generate a temporary pulse of editor production. This may reduce prolonged nuclease exposure and improve safety.
LNPs are highly scalable from a manufacturing perspective and have demonstrated strong liver delivery after systemic administration. As a result, they are central to many in vivo editing programs targeting hepatic disease.
However, conventional LNP systems often show strong liver tropism, making delivery to extrahepatic tissues more difficult. Endosomal escape also remains inefficient, meaning that only a fraction of internalized cargo reaches the cytoplasm. Current research is therefore focused on lipid chemistry optimization, organ-selective nanoparticles, and intracellular trafficking improvements.
Polymeric Nanoparticles
Polymeric systems provide a highly modular alternative to lipids. Synthetic or semi-synthetic polymers can condense nucleic acids, shield cargo during circulation, and be engineered for controlled release or tissue targeting.
The principal attraction of polymeric systems lies in tunability. Charge density, hydrophobicity, biodegradability, branching structure, and ligand decoration can all be adjusted to influence pharmacology. This makes polymer systems especially interesting for custom indications where standard LNPs are suboptimal.
Historically, however, some polymer systems have faced toxicity, inflammatory responses, or inconsistent reproducibility. Translation therefore depends on balancing engineering flexibility with robust manufacturing and favorable safety profiles.
Ligand-Conjugated and Targeted Delivery Systems
A major goal in the field is cell-selective delivery. Rather than relying on passive biodistribution, ligand-conjugated systems use molecules such as sugars, peptides, antibodies, or receptor-binding domains to direct cargo into specific cell populations.
This approach has already proven valuable in liver targeting through receptor-mediated uptake mechanisms and may become increasingly important for immune cells, tumors, and extrahepatic organs. If successful, targeted systems could improve potency while lowering systemic exposure and off-target toxicity.
The long-term significance of ligand-based targeting may be substantial, especially for editors requiring low-dose precision delivery.
Extracellular Vesicles and Hybrid Platforms
Extracellular vesicles, including exosomes and engineered membrane particles, represent an emerging biologically inspired delivery strategy. Because they are naturally involved in intercellular communication, they may offer improved compatibility and lower immunogenicity compared with some synthetic systems.
These platforms are being explored for RNA delivery, protein delivery, and potentially CRISPR ribonucleoprotein transport. Hybrid systems that combine vesicle membranes with synthetic nanoparticles may also capture the advantages of both modalities.
Although still early in development, vesicle-based systems are especially intriguing for CNS delivery, repeat administration, and sensitive immune contexts.
Comparative Overview of Gene Editing Delivery Platforms
| Platform | Typical Cargo | Major Strength | Key Limitation | Leading Use Cases |
|---|---|---|---|---|
| AAV | DNA expression cassette | Efficient transduction | Cargo size, immunity | Eye, muscle, localized tissues |
| LNP | mRNA + gRNA | Transient, scalable | Liver bias | Liver editing |
| Electroporation | RNP / DNA | High ex vivo control | Not systemic | Stem cells, T cells |
| Polymer NP | RNA / DNA | Highly tunable | Translation complexity | Experimental tissue targeting |
| Ligand Conjugates | RNA/editor fragments | Precision targeting | Payload constraints | Cell-specific delivery |
| Extracellular Vesicles | RNA/protein | Biocompatibility | Early-stage maturity | CNS / immune research |
Delivery Requirements for Different Editing Modalities
Not all editors impose the same delivery burden. Classical CRISPR nucleases are comparatively compact and can be delivered as protein-RNA complexes, mRNA systems, or DNA vectors. Base editors are larger fusion proteins that require efficient transient expression and careful dose balancing.
Prime editors are among the most demanding platforms. They typically combine a Cas nickase with reverse transcriptase and require specialized pegRNAs. Their larger cargo size and multi-component coordination make delivery especially challenging. As a result, advances in delivery science may be particularly decisive for clinical prime editing.
This illustrates an important principle: the therapeutic viability of an editing modality often depends as much on deliverability as on molecular elegance.
Biological Barriers That Still Limit Clinical Translation
Several persistent barriers continue to define the field. Endosomal trapping remains a major inefficiency for many nanoparticle systems. Cargo may enter cells successfully but fail to escape into the cytoplasm. Tissue specificity is another challenge, particularly beyond the liver.
Immune recognition remains a concern for both viral and non-viral platforms. Patients may react to capsid proteins, lipid components, bacterial Cas enzymes, or repeated exposure regimens. Manufacturing consistency also becomes more complex as delivery systems increase in sophistication.
Finally, dose remains a central issue. Large editing cargos or poorly efficient systems may require higher doses, which can narrow safety margins and increase cost.
What Is Driving the Next Phase of Innovation
The next generation of delivery platforms is focused on precision rather than brute force. Organ-selective nanoparticles a re being engineered to reach lung, spleen, bone marrow, muscle, and CNS tissues. Large editors are being split into smaller components for easier packaging. Ribonucleoprotein delivery is being optimized to provide rapid but short-lived editing pulses.
Smart materials that respond to pH, enzymes, or intracellular redox environments may improve release kinetics. At the same time, computational methods and machine learning are being used to predict lipid performance, capsid behavior, and tissue tropism.
These developments suggest that delivery systems are becoming programmable technologies in their own right.
Safety Considerations in Clinical Trials
Clinical translation requires more than demonstrating editing efficiency. Investigators must monitor unintended sequence changes, large deletions, chromosomal rearrangements, vector-related toxicity, immune responses, and long-term persistence of edited cells.
Transient delivery approaches may reduce some risks associated with persistent expression, but they can introduce their own challenges in dosing and repeat administration. Safety therefore depends on integrated optimization of editor design, delivery chemistry, route of administration, and patient selection.
As regulators gain more experience with these therapies, analytical characterization of both cargo and carrier will become increasingly important.
Discussion
Gene editing medicine is evolving from a molecular discovery discipline into a translational engineering field. Highly capable editors already exist for cutting DNA, rewriting bases, or installing precise sequence changes. The central question is increasingly how to deploy them safely and reproducibly in real patients.
This shift places delivery science at the center of therapeutic value creation. Companies and research groups that solve biodistribution, tissue selectivity, manufacturing scalability, and tolerability may unlock the broadest clinical impact. In many cases, a modest editor paired with an exceptional delivery platform may outperform a theoretically superior editor that cannot reach target cells efficiently.
The field should therefore be understood not as editor versus editor, but as complete therapeutic systems competing on efficacy, safety, convenience, and cost.
Future Directions
Future progress described in the referenced literature points toward tissue-specific delivery, repeat-dose compatible platforms, extrahepatic editing, lower immunogenicity systems, and increasingly modular cargo architectures. These advances will be especially important for diseases requiring treatment in heart, brain, muscle, or diffuse systemic tissues.
Another likely direction is convergence between gene editing and precision medicine. Patient genotype, tissue biomarkers, immune profile, and disease stage may eventually guide individualized selection of editor type, guide design, and delivery modality.
The long-term success of the field will depend on transforming powerful molecular tools into predictable medicines.
Conclusion
Gene editing has moved decisively into the clinic, but therapeutic success now depends on more than the editor itself. Clinical translation requires delivery systems that can transport complex molecular cargo with precision, safety, and scalability.
Ex vivo approaches have already demonstrated durable benefit in hematology and oncology. In vivo systems, especially nanoparticles and engineered viral vectors, are opening the path toward broader organ targeting and larger patient populations.
The next era of gene editing will be defined by the marriage of molecular precision with delivery intelligence. Those platforms that master both will shape the future of genomic medicine.
Explore related insights
- Prime Editing: Advances in Human Gene Therapy
- Past, Present, and Future of CRISPR Genome Editing Technologies
- Trends in Clinical Genetic Testing
- Single-Cell Multi-omics Technologies
- Integrating Genomics into Multimodal EHR Foundation Models